































There is a connection between bone fractures, bone loss and Celiac disease. There is a connection between gastrointestinal disea
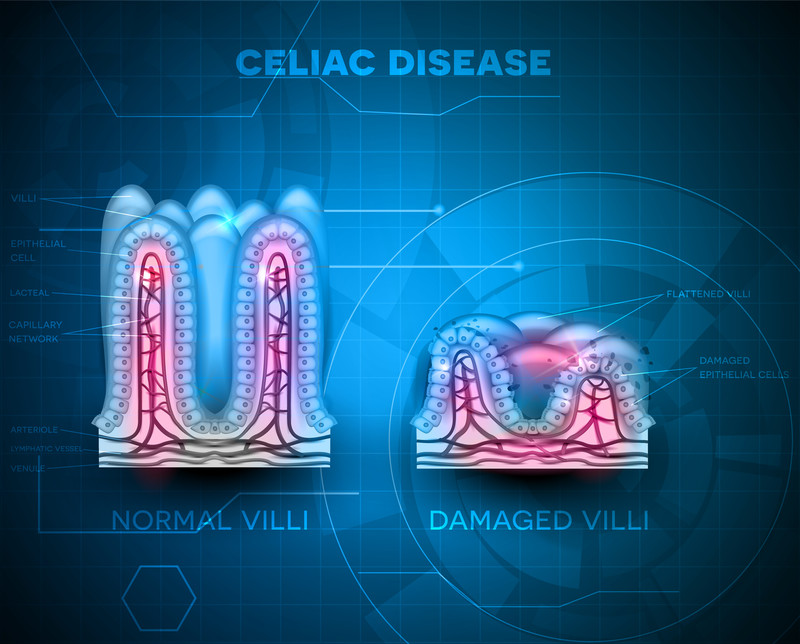
According to the Celiac Disease Foundation, celiac disease is a serious genetic autoimmune disorder where the ingestion of gluten leads to damage in the small intestine. It is estimated to affect 1 in 100 people worldwide. Two and one-half million Americans are undiagnosed and are at risk for long-term health complications. Studies have shown and confirmed that celiac disease is over four times more common today than it was 50 years ago and this is leading to a vast array of health complications including what three studies say: A greater risk in breaking a bone.
Despite these numbers and more people at risk, researchers still struggle to understand the best ways to help patients.
Moving beyond a gluten-free strategy
In October of 2019, a study published in the journal Frontiers in nutrition (1) made the suggestion that doctors need to move beyond the gluten-free diet recommendation for patients with celiac diseases. Here is what they wrote:
“Gluten free diet is the only available treatment for celiac disease. Patients with celiac disease who do not adhere to a strict gluten-free diet have been found to have complications involving nutritional deficiencies, increased risk of bone fractures, increased risk of mortality, and certain types of cancers. Complete removal of gluten from the diet in a patient with celiac disease often results in symptomatic, serologic, and histologic remission. However, strict compliance with the diet is challenging.”
What the researchers suggest is that there needs to be more than diet recommendations as many patients, unknowingly accidentally eat gluten products and this can set them back considerably. Other factors to boost the patient’s immune response to celiac disease is needed.
Malabsorption of calcium and vitamin D is a focus
Vitamin D is important because it’s a crucial part of calcium absorption. Even if you take the right amount of calcium, it won’t be properly absorbed without the right amount of Vitamin D. A lack of Vitamin D can lead to poor bone health. In addition to its benefits for your bone health, Vitamin D has also been found to be crucial to boosting and maintaining your immune system.
The amount of Vitamin D adults need tends to be around 600 to 800 IUs, but some research has found that adults might need up to 2000 IUs for the most benefits. But what is the best way to get all of this Vitamin D? Most food does not contain Vitamin D naturally except for fatty fish, but many products such as milk, juice, or cereal are fortified with some of your daily required amount. Despite this, the best way to get Vitamin D is through sunlight. Just being outdoors between five to 30 minutes a day is enough for your body to produce its own Vitamin D.
Controversy
There is some controversy in regard to vitamin D and celiac disease. Some researchers suggest that vitamin D will not help some people diagnosed with celiac disease. Other suggest that doctors need a better understanding of the relationship between vitamin D and celiac disease and that this understanding needs to be adapted into clinic use.
An April 2020 in the journal Nutrients, (2) study sought to explain the role of vitamin D in managing Celiac disease.
“studies have investigated possible roles of vitamin D as a key modulator of inflammation and immune mechanisms and of the intestinal mucosa barrier. (Gut inflammation) In this regard, vitamin D has been considered as a factor that affects different conditions such as immune-mediated diseases.
The new emerging role of vitamin D and its involvement in immune modulation has led it to be considered as a possible key factor involved in celiac disease onset. Celiac disease is a chronic immune-mediated enteropathy (disease) of the small intestine that is triggered by dietary gluten protein exposure in individuals who are genetically predisposed. However, along with gluten, other environmental factors are also involved in celiac disease onset. . .although there remains a lack of studies aimed at contextualizing the role of vitamin D on celiac disease.”
The researchers concluded that studying and evaluating vitamin D should be part of new celiac disease prevention strategies.
Clinically, we have seen a connection between vitamin D deficiency and celiac disease. Researchers have too.
Vitamin D and celiac disease connections
In June 2018, researchers from the Professional Advisory Council for the Canadian Celiac Association published findings in the journal Canadian family physician (3) that suggested certain guidance recommendations on monitoring bone health in celiac disease patients. What they were looking for was treatments that may help. Addressing malabsorption of calcium and vitamin D was the focus.
“Bone health can be negatively affected in both adults and children with celiac disease owing to the inflammatory process and malabsorption of calcium and vitamin D. Most adults with symptomatic celiac disease at diagnosis have low bone mass. Bone mineral density should be tested at diagnosis and at follow-up, especially in adult patients.
Vitamin D levels should be measured at diagnosis and annually until they are normal. In addition to a strict gluten-free diet, supplementation with calcium and vitamin D should be provided and weight-bearing exercises encouraged.”
A December 2018 study published in the Scandinavian journal of gastroenterology (4) focused on younger patients with celiac disease and the concerns of adequate calcium and vitamin D supplementation. Here doctors in the United Kingdom questioned guidelines that do not support routine investigation of bone loss in younger patients when clearly the problem of bone loss will manifest itself in their later life. They argued: “Early identification may improve motivation to comply with gluten-free diet and allow adequate calcium and vitamin D supplementation to reduce risk of fracture later in life.”
Untreated Celiac disease and substantial risk of osteoarthritis and osteoporosis
Once diagnosed calcium and vitamin D supplementation can help. But what if patients ignore their symptoms or are undiagnosed?
Researchers in Italy published their findings in the October 2018 issue of the United European gastroenterology journal (5) suggesting up to 75% of patients with untreated celiac disease show up at doctor’s offices with osteopenia or osteoporosis. The aim of their study was to evaluate the prevalence of bone mineral density alterations at diagnosis and risk factors associated with osteoporosis in these Celiac disease patients.
What is important here is the patients who were being studied.
A total of 214 adult patients (average age 38 years old; 7 out of 10 were female)
These patients had newly diagnosed with celiac disease and underwent a DEXA bone scan.
39.7% had normal Bone Mineral Density
42.5% had osteopenia
17.8% had osteoarthritis
Sixty percent of the patients in this study, average age 38 years old, newly diagnosed with celiac disease had bone deformity and bone loss.
A recent study published in The Journal of clinical endocrinology and metabolism (6) led by a research team from Massachusetts General Hospital found that bone fractures were almost twice as common in individuals with a clinically diagnosed celiac disease as in those without the disease. Especially hip fractures, where the research team reported a 69% increase in the risk of hip fracture.
When you have Celiac disease and gastrointestinal disease
According to the Celiac Disease Foundation, “At least 20% of individuals with Celiac disease continue to have symptoms on a gluten-free diet. Other estimates show that more than one third of celiac disease patients have altered gut motility or “IBS-like” symptoms. Likewise, about 25% of those with non-celiac gluten sensitivity also continue to have symptoms on a gluten-free diet. While continued gluten ingestion is the most common cause of persistent symptoms in both populations, a dual diagnosis of irritable bowel syndrome (IBS) is also common.”
This is the danger of relying on the “magic bullet theory,” of treating anything. Patients with celiac disease will follow a strict gluten-free diet yet continue to suffer from symptoms. The symptoms are caused by other gastrointestinal disease
In November 2018, researchers wrote in the Journal of Bone Metabolism: (7)
Patients with gastrointestinal disease are at risk for osteopenia or osteoporosis, which can lead to fractures. Although these patients may be at risk from a young age, gastroenterologists often overlook this fact in practice.
There are well-known GI diseases associated with osteopenia and osteoporosis, such as the post-gastrectomy state, inflammatory bowel disease (IBD), and celiac disease. As there is an increase in the prevalence of IBD patients, newly diagnosed celiac disease in adulthood, and gastric cancer survivors following gastrectomy, bone disease in these patients becomes an important issue.
We have confirmed that the prevalence of osteoporosis and fractures in each of these diseases is high.
Intensive surveillance and management are needed to ensure that these patients attain peak bone mass for age and sex to prevent fractures.
Treatment – the role of probiotics?
In September 2020, researchers summarized the existing role of probiotics on celiac disease.(8)
“To date, the only available treatment for celiac disease patients is a life-lasting gluten-free diet. Lack of adherence to the gluten-free diet leads to a significant risk of adverse health consequences. Food cross-contamination, nutritional imbalances, and persistent gastrointestinal symptoms are the main concerns related to gluten-free diet.
Moreover, despite rigid compliance to gluten-free diet, patients struggle in achieving a full restoring of the gut microbiota, which plays a role in the nutritive compounds processing, and absorption. Pivotal studies on the supplementation of gluten-free diet with probiotics, such as Bifidobacterium and Lactobacilli, reported a potential to restore gut microbiota composition and to pre-digest gluten in the intestinal lumen, reducing the inflammation associated with gluten intake, the intestinal permeability, and the cytokine and antibody production (simply inflammation). These findings could explain an improvement in symptoms and quality of life in patients treated with gluten-free diet and probiotics.”
At the Magaziner Center, we believe in treating digestive disorders with intensive surveillance and management at the source. We approach healthcare from a holistic standpoint and look at the entire body and how it is functioning, rather than looking only at the gastrointestinal tract.
Through specialized blood and stool testing, we often find abnormal digestion or assimilation, imbalance in the flora or fatty acid metabolism and leaky guy syndrome or increased intestinal permeability that is triggering the problem. Once these imbalances are addressed, we see tremendous healing and improvement in our patients.
If you would like to explore more information, please contact our office so we can start a conversation with you.
Related articles:
Low Testosterone and Depression
Celiac Disease
Low Testosterone and Depression
References:
1 Pinto-Sanchez MI, Bai JC. Toward New Paradigms in the Follow Up of Adult Patients With Celiac Disease on a Gluten-Free Diet. Front Nutr. 2019 Oct 1;6:153. doi: 10.3389/fnut.2019.00153. PMID: 31632977; PMCID: PMC6781794.
2 Vici G, Camilletti D, Polzonetti V. Possible Role of Vitamin D in Celiac Disease Onset. Nutrients. 2020 Apr 10;12(4):1051. doi: 10.3390/nu12041051. PMID: 32290294; PMCID: PMC7231074.
3 Duerksen D, Pinto-Sanchez MI, Anca A, et al. Management of bone health in patients with celiac disease: Practical guide for clinicians. Can Fam Physician. 2018;64(6):433-438.
4 Pritchard L, Wilson S, Griffin J, Pearce G, Murray IA, Lewis S. Prevalence of reduced bone mineral density in adults with coeliac disease–are we missing opportunities for detection in patients below 50 years of age?. Scandinavian journal of gastroenterology. 2018 Nov 26:1-4.
5 Galli G, Lahner E, Conti L, Esposito G, Sacchi MC, Annibale B. Risk factors associated with osteoporosis in a cohort of prospectively diagnosed adult coeliac patients. United European Gastroenterol J. 2018;6(8):1161-1168.
6 Heikkila K, Pearce J, Maki M, Kaukinen K. Celiac disease and bone fractures: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2015 Jan;100(1):25-34. doi: 10.1210/jc.2014-1858.
7 Oh HJ, Ryu KH, Park BJ, Yoon BH. Osteoporosis and Osteoporotic Fractures in Gastrointestinal Disease. Journal of bone metabolism. 2018 Nov 1;25(4):213-7.
8 Marasco G, Cirota GG, Rossini B, Lungaro L, Di Biase AR, Colecchia A, Volta U, De Giorgio R, Festi D, Caio G. Probiotics, Prebiotics and Other Dietary Supplements for Gut Microbiota Modulation in Celiac Disease Patients. Nutrients. 2020 Sep;12(9):2674.
Recent Comments